


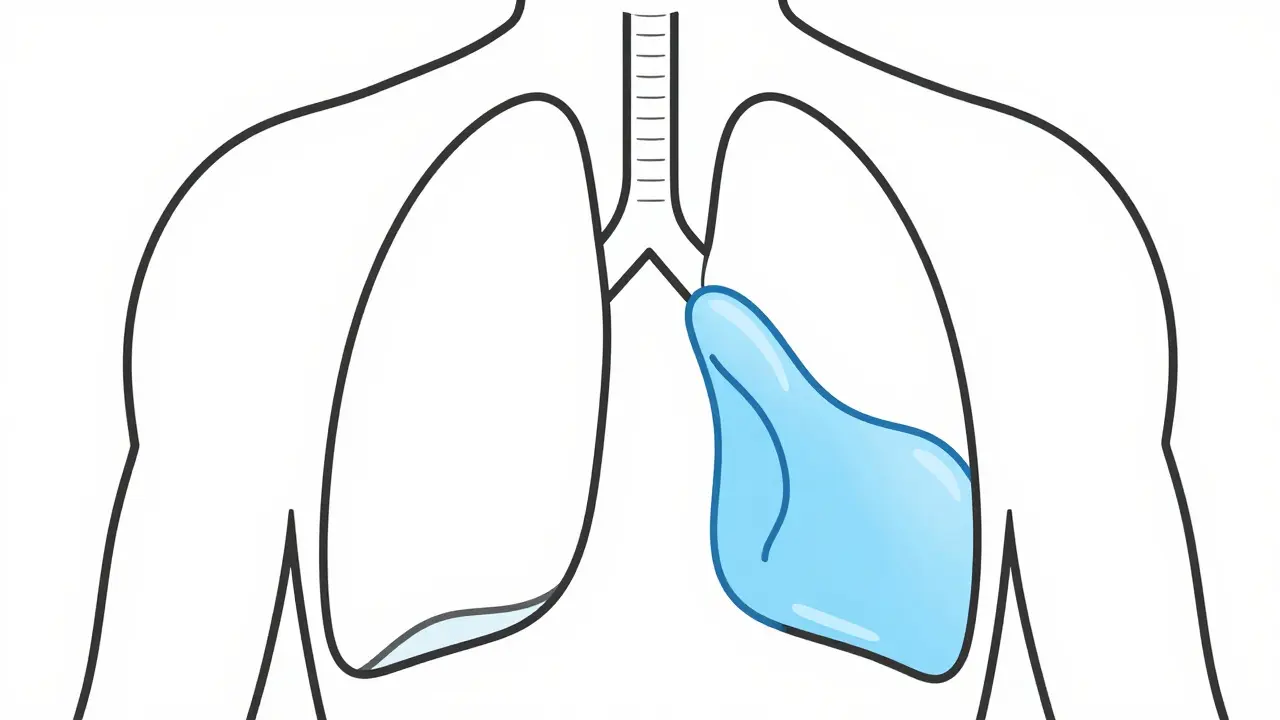
Imagine trying to take a deep breath, but it feels like there is a heavy wall stopping your lungs from expanding. That is exactly what happens during a pleural effusion is an abnormal buildup of fluid in the pleural space, the thin area between the two layers of the pleura that line your lungs and chest cavity. When fluid fills this gap, it pushes against the lung, making every breath a struggle. While it can feel alarming, the key to recovery isn't just removing the liquid-it is figuring out why it's there in the first place.
What Exactly Causes the Fluid Buildup?
Not all pleural effusions are the same. Doctors split them into two main groups: transudative and exudative. Think of it as a difference between a "leak" and an "inflammation."
Transudative effusions happen when the balance of pressure in your blood vessels is off. Fluid simply leaks out of the capillaries because of high pressure or low protein levels. For instance, congestive heart failure is the biggest culprit here, causing about 90% of these cases. When the heart can't pump effectively, fluid backs up into the lungs. Other causes include cirrhosis of the liver or nephrotic syndrome, where the body loses protein through urine, making it harder for blood vessels to hold onto fluid.
On the flip side, exudative effusions are more aggressive. They happen when the lining of the lung becomes damaged or inflamed, letting proteins and cells leak through. Pneumonia is a very common trigger, accounting for 40-50% of exudative cases. However, malignancy-like lung cancer-is also a major cause, representing 25-30% of these instances. Other triggers include pulmonary embolisms and tuberculosis.
| Feature | Transudative | Exudative |
|---|---|---|
| Main Cause | Pressure imbalances (e.g., Heart Failure) | Inflammation/Damage (e.g., Pneumonia, Cancer) |
| Fluid Nature | Clear, low protein | Cloudy, high protein/cells |
| Typical Trigger | Systemic issues (Heart, Liver, Kidney) | Local lung issues or malignancy |
| Key Metric | Low Protein/LDH ratio | High Protein/LDH ratio |
The Gold Standard: Light's Criteria
How do doctors know which type of effusion they are dealing with? They use a set of rules called Light's criteria. Established in 1972, these rules are still the gold standard because they are incredibly accurate. To call an effusion "exudative," the fluid must meet at least one of these three markers:
- The ratio of protein in the pleural fluid to protein in the blood is greater than 0.5.
- The ratio of lactate dehydrogenase (LDH) in the fluid to LDH in the blood is greater than 0.6.
- The LDH level in the fluid is more than two-thirds of the upper limit of normal for blood LDH.
If the fluid doesn't meet these, it's usually a transudate. This distinction is vital because treating a heart failure leak with the same tools used for a cancerous growth would be ineffective and potentially dangerous.

How Thoracentesis Works
When the fluid becomes too heavy for the lungs to handle, doctors perform a thoracentesis. This is a procedure where a needle or catheter is inserted into the pleural space to drain the liquid. It serves two purposes: it helps you breathe better immediately (therapeutic) and gives doctors a sample to test (diagnostic).
In the past, this was often done by a doctor feeling for the right spot. Today, that's outdated. Modern care requires ultrasound guidance. Using a probe to see exactly where the fluid is reduces complications-like accidentally puncturing a lung (pneumothorax)-by nearly 80%. Typically, the needle goes in around the 5th to 7th rib in the mid-axillary line. While they might take a small amount for testing, they can remove up to 1500mL in one go to provide instant relief.
However, it's not without risk. Some patients experience a pneumothorax or a rare condition called re-expansion pulmonary edema, where the lung refills too quickly after being compressed. This is why the procedure must be done by trained professionals who understand the pressure dynamics of the chest.
Stopping the Fluid from Coming Back
Draining the fluid is like bailing water out of a sinking boat. If you don't patch the hole, the boat will just fill up again. This is why recurrence prevention is focused entirely on the root cause.
For people with heart failure, the solution is medical management. Using diuretics to flush excess fluid and medications like ACE inhibitors helps keep the fluid from returning. When guided by specific biomarkers like NT-pro-BNP, recurrence rates can drop from 40% down to 15%.
Malignant effusions are trickier. They have a 50% chance of returning within just 30 days of a single drainage. To stop this, doctors use pleurodesis. This involves irritating the pleural lining-often using talc or chemical agents-so the two layers of the pleura stick together, effectively closing the space where fluid would collect. While it works in 70-90% of cases, it can be painful.
A more modern alternative for cancer patients is the indwelling pleural catheter. This is a small, permanent tube that stays in the chest, allowing the patient to drain the fluid safely at home. This shift has significantly cut down hospital stays, reducing them from over a week to just a couple of days.
If the effusion is caused by pneumonia (a parapneumonic effusion), the priority is aggressive antibiotics and drainage. If the fluid becomes too thick or infected (empyema), surgical intervention becomes necessary to prevent permanent lung scarring.
How do I know if I have a pleural effusion?
The most common sign is shortness of breath, especially when lying flat. You might also experience a dry cough or a sharp chest pain that gets worse when you breathe deeply (pleuritic pain). However, because these symptoms mimic other lung issues, a chest X-ray or ultrasound is the only way to confirm the presence of fluid.
Is thoracentesis painful?
The procedure involves a local anesthetic to numb the skin and the chest wall, so the actual needle insertion is usually just a pinch. Some patients feel a strange sensation or mild pressure as the fluid is removed. Using ultrasound guidance makes the process quicker and more precise, which generally improves the overall experience.
Can a pleural effusion go away on its own?
It depends on the cause. Small effusions caused by a mild infection might resolve with antibiotics. However, those caused by heart failure or cancer will not disappear without treating the underlying disease. If left untreated, malignant effusions can severely limit survival times, making medical intervention critical.
What is the difference between an effusion and pneumonia?
Pneumonia is an infection of the lung tissue itself (the alveoli), while a pleural effusion is fluid outside the lung, in the space surrounding it. That said, pneumonia often causes a pleural effusion, creating a combined condition called a parapneumonic effusion.
How long does it take to recover from pleurodesis?
Recovery varies, but most patients experience some chest soreness or pain for several days following the procedure. The goal is to create a permanent seal, and once that's achieved, the relief from no longer needing frequent drainages usually outweighs the temporary discomfort.
Next Steps and Troubleshooting
If you or a loved one are dealing with this condition, the first step is always a precise diagnosis. Don't settle for just "removing the fluid." Ask your medical team about the fluid analysis results: was it a transudate or an exudate? What did the LDH and protein levels show?
For those managing chronic recurrence, specifically with malignancy, discuss the pros and cons of a permanent catheter versus a one-time pleurodesis. The catheter offers more independence and fewer hospital visits, while pleurodesis aims for a permanent "fix." If you are recovering from a heart-related effusion, keep a strict log of your daily weight and sodium intake, as sudden weight gain is often the first sign that fluid is building up again before you even feel breathless.