



When you’re managing asthma, an inhaled corticosteroid (ICS) is often the most effective tool you have. It doesn’t cure asthma, but it stops the inflammation that makes your airways tight, swollen, and reactive. For millions of people, this daily puff from an inhaler means fewer attacks, less wheezing, and the ability to live without constantly worrying about breathing. But here’s the catch: even though these medications are lifesavers, they’re not harmless. Side effects are real - and many people don’t know how to spot them, prevent them, or when to ask for help.
What Are the Most Common Side Effects?
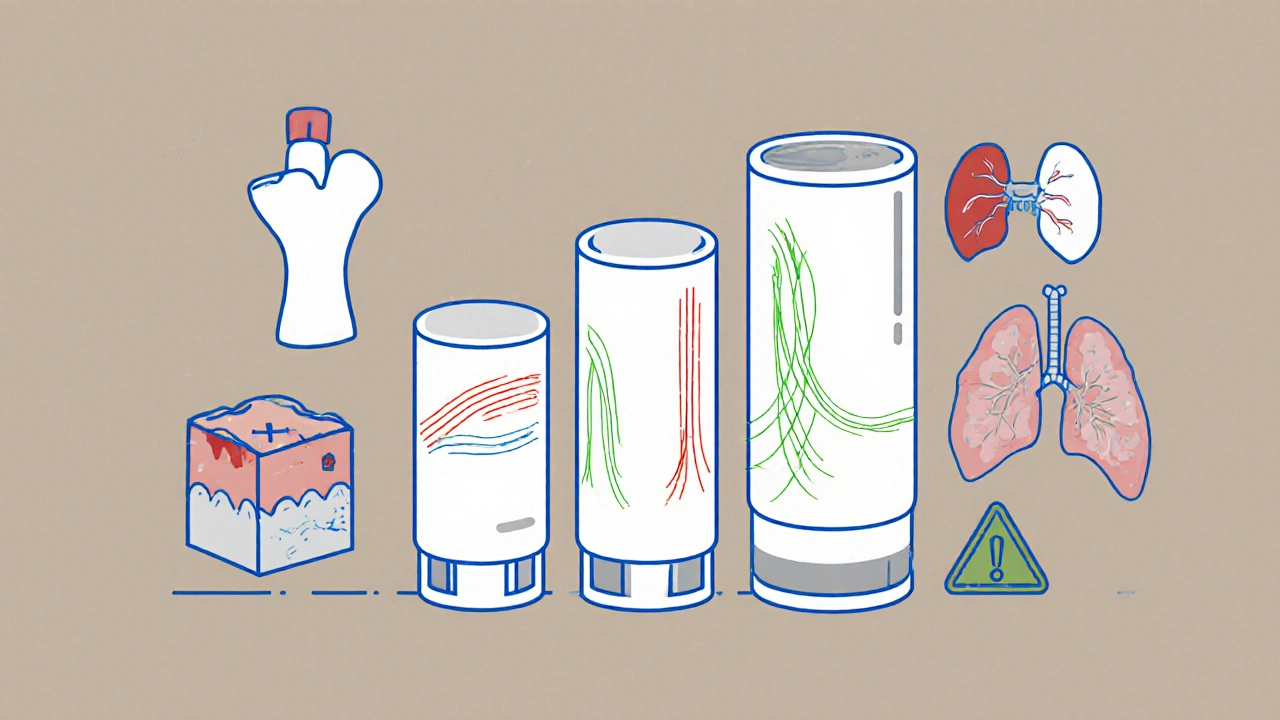
Most side effects from inhaled steroids aren’t scary - but they’re annoying enough to make people stop taking their medicine. The top three? Oral thrush, hoarse voice, and throat irritation. Thrush looks like white patches in your mouth or throat. It’s not dangerous, but it hurts to swallow and can feel like you’ve got cotton in your mouth. Voice changes - sounding hoarse or raspy - happen because the steroid settles on your vocal cords. And throat irritation? That scratchy, tickly feeling after you inhale? That’s the medication sitting where it shouldn’t.These aren’t random. They happen because the drug doesn’t just go to your lungs. A big chunk sticks to your mouth and throat. That’s why rinse and spit after every use isn’t optional - it’s essential. Studies show rinsing cuts thrush risk by more than half. Use water, not just swishing. Spit it out. Don’t swallow it. And if you’re using a metered-dose inhaler (the kind with a canister), always use a spacer. It’s a simple plastic tube that holds the puff so you breathe it in slowly. Without one, only 10-20% of the dose reaches your lungs. With one? It jumps to 60-80%. That means less drug sitting in your mouth - and fewer side effects.
When Side Effects Go Deeper: Systemic Risks
The real concern isn’t just the throat. It’s what happens when the steroid gets into your bloodstream. That’s called systemic absorption. And it’s dose-dependent. The higher the dose, the more likely you are to run into problems.At low doses - under 200 mcg of fluticasone or 400 mcg of beclomethasone per day - the risk of serious side effects is very low. But if you’re on more than 500 mcg of fluticasone daily for months or years, things change. Your body’s natural cortisol production can slow down. That’s adrenal suppression. It doesn’t mean you’ll collapse, but you might feel tired all the time, get sick more easily, or struggle to handle stress like an infection or surgery. If you’ve been on high-dose ICS for over six months, your doctor should check your adrenal function.
Other risks include thinning skin, which can lead to easy bruising - especially in older adults. One study found that people on high-dose ICS for five years or more had a 34% chance of noticeable skin thinning. That’s nearly seven times higher than those on low doses. Bone density can drop too, especially in postmenopausal women and men over 65. If you’re on more than 750 mcg/day for five years, a bone scan is recommended.
And then there’s pneumonia. For people over 65, high-dose ICS increases the risk by nearly 70%. That’s not a small number. It’s why doctors now avoid pushing doses higher than needed - especially in older patients.
Which Inhaler Is Safest?
Not all inhaled steroids are the same. Some are designed to be absorbed less into your bloodstream. Ciclesonide and mometasone, for example, have very low systemic bioavailability - as little as 2-5%. That means they work just as well in your lungs but cause fewer side effects elsewhere. Budesonide is also gentler than fluticasone. One study found fluticasone at 500 mcg/day carried nearly three times the risk of adrenal suppression compared to the same dose of budesonide.So if you’re on high-dose fluticasone and having side effects, ask your doctor if switching to budesonide or ciclesonide could help. You might get the same asthma control with less risk.
Special Groups: Kids, Seniors, and Pregnant People
Children on ICS do experience a slight slowdown in growth - about 0.7 cm per year on average. But long-term studies show they catch up. Final adult height isn’t affected if doses stay below 400 mcg/day of beclomethasone equivalent. But if a child is on more than 800 mcg/day? That’s a red flag. Higher doses raise the risk of cataracts and other issues.For older adults, the risks are different. Fractures become more likely. A 2023 study showed ICS doses above 500 mcg/day increased fracture risk by 31%. That’s why doctors now check bone health in seniors on long-term steroids.
Pregnant women? Budesonide is the safest choice. It’s been studied the most in pregnancy and has the best safety record. Fluticasone is less proven. If you’re pregnant and using asthma medication, don’t stop - but do talk to your doctor about switching to budesonide if you’re not already on it.
How to Monitor Your Health
You can’t manage what you don’t measure. Here’s what you should track:- Every 3-6 months: Ask your provider to check your inhaler technique. Up to 60% of people use their inhaler wrong - and that’s why side effects happen.
- Annually: If you’re over 65 and on high-dose ICS, get your skin checked for thinning or bruising.
- Every 5 years: If you’ve been on over 750 mcg/day for five years, get a bone density scan.
- If you feel unusually tired: Ask for a salivary cortisol test. Levels below 3 mcg/dL suggest your adrenal glands are struggling.
- Track your symptoms: Are you using your rescue inhaler more than twice a week? Are you waking up at night? If yes, your maintenance dose might be too low - or your technique is off.
New tech is helping too. Smart inhalers now track when you use them and even detect if you’re using the right technique. Some can send alerts to your phone if you forget to rinse or use the spacer. These aren’t gimmicks - they’re tools that reduce side effects by improving adherence and technique.
What You Can Do Right Now
You don’t have to wait for your next appointment to lower your risk. Here’s your action plan:- Use a spacer - always - if you have a metered-dose inhaler.
- Rinse your mouth and spit after every puff. No exceptions.
- Ask your doctor if you’re on the lowest effective dose. Many people stay on high doses long after their asthma is under control.
- Switch if needed. If you’re on fluticasone and have side effects, ask about budesonide or ciclesonide.
- Keep a side effect journal. Note any voice changes, thrush, bruising, or fatigue. Bring it to your next visit.
Remember: the goal isn’t to avoid steroids. It’s to use them wisely. Asthma control saves lives. But uncontrolled asthma kills. The right dose, used correctly, keeps you safe on both fronts.
What’s Next for Asthma Treatment?
The future is moving away from high-dose steroids. New biologic drugs - like dupilumab - target specific parts of the immune system that cause inflammation. In severe asthma, they’ve cut ICS use by 70%. That’s huge. These aren’t for everyone - they’re for people with high eosinophil levels or severe symptoms despite high-dose ICS. But they’re changing the game.Even newer ICS drugs are in development. One, called AZD7594, showed 90% less adrenal suppression than fluticasone in early trials. It’s not on the market yet, but it’s a sign that safer steroids are coming.
For now, the best tool you have is knowledge. Know your dose. Know your technique. Know your body. And don’t be afraid to ask your doctor: "Is this the lowest dose I need?"
Can inhaled steroids cause weight gain?
Inhaled corticosteroids rarely cause weight gain because the dose is so low and mostly stays in the lungs. Unlike oral steroids, which flood your system, inhaled versions deliver less than 10% of the dose into your bloodstream. Weight gain is more common with high-dose oral steroids taken for weeks or months. If you’re gaining weight on your inhaler, it’s likely due to other factors - diet, activity level, or another medication.
How long does it take for side effects to go away after stopping?
Local side effects like thrush or hoarseness usually clear up within days of rinsing better or switching inhalers. Systemic effects like adrenal suppression take longer - weeks to months - depending on how long and how high your dose was. Your body needs time to restart its natural cortisol production. Never stop your inhaler suddenly. Always work with your doctor to taper down safely.
Do I need to take breaks from my steroid inhaler?
No. Asthma is a chronic condition. Stopping your inhaler, even for a few days, can cause your airways to become inflamed again and trigger an attack. The goal is to use the lowest effective dose daily, not to take breaks. Skipping doses increases your risk of flare-ups more than it reduces side effects.
Can children use steroid inhalers safely long-term?
Yes, when used correctly. Studies tracking children for over a decade show that standard doses of inhaled steroids (under 400 mcg/day of beclomethasone equivalent) cause only a tiny, temporary delay in growth - about 0.7 cm per year. Most kids catch up by adulthood. The bigger risk is uncontrolled asthma, which can affect lung development. The benefits far outweigh the risks at recommended doses.
What should I do if I think my inhaler is causing side effects?
Don’t stop taking it. Instead, schedule a visit with your doctor or asthma nurse. Bring your inhaler and show them how you use it. They can check your technique, assess whether your dose is still necessary, and possibly switch you to a safer steroid. Keep a log of symptoms - when they started, how often they happen, and if they improve after rinsing. That helps them make the best decision.
Comments
8 Comments
Justin Hampton
Look, I get that doctors push these inhalers like they’re candy, but half the people I know who’ve been on them for years look like they’ve been through a war-bruises everywhere, voice like a rusty gate, and they’re still wheezing. Why aren’t we talking about how these drugs are just Band-Aids on a bullet wound? I stopped mine after three years and my asthma didn’t get worse-it got better because I finally started breathing right, not just puffing chemicals.
Pooja Surnar
lol u guys are so paranoid abt side effects 😂 like wtf u think ur lungs are made of glass? i was on fluticasone for 8 yrs n never had thrush or bruising, but my asthma? gone. u think u r so smart with ur 'rinse and spit' but half of u probably just skip doses n blame the inhaler. grow up. if ur scared of side effects, dont use it. but dont act like ur a doctor just bc u read one article.
Sandridge Nelia
This is such a helpful breakdown! 🙌 I switched from fluticasone to budesonide last year after my voice got raspy all the time-game changer. Also, using a spacer changed everything. I didn’t realize how much I was wasting the dose until I saw the difference. If you’re on a high dose and still having issues, ask about a smart inhaler-they actually track if you rinse! My app even reminds me. So much less guilt now 😊
Mark Gallagher
Let’s be clear: if you’re using an inhaler without a spacer, you’re not just risking side effects-you’re wasting medical resources. The CDC recommends spacers for all metered-dose inhalers. The fact that 60% of patients use them incorrectly isn’t a failure of the medication-it’s a failure of healthcare education in this country. We need mandatory inhaler training in schools. This isn’t optional. This is basic science.
Wendy Chiridza
I’ve been on low-dose budesonide for 12 years and never had thrush or voice issues because I rinse every single time. I also track my rescue inhaler use in a notebook. If I’m using it more than twice a week, I call my doctor. Simple. No drama. Just accountability. Also, for anyone worried about weight gain-nope, not from this. I gained 15 lbs after I stopped exercising, not because of my inhaler. Don’t confuse correlation with causation
Pamela Mae Ibabao
Okay but let’s talk about the real elephant in the room-why do we still treat asthma like it’s a 1990s problem? We have biologics now that can cut steroid use by 70% and yet most docs won’t even mention them unless you’re on the verge of dying. It’s not that these inhalers are bad-it’s that the system is stuck in the past. I’ve seen patients on 1000 mcg of fluticasone who could’ve been on dupilumab for $30 a month. That’s not healthcare. That’s negligence dressed up as caution.
Gerald Nauschnegg
Wait, so if I’m on high-dose ICS and I’m 68, I need a bone scan every 5 years? And a skin check? And a cortisol test if I’m tired? That’s like five different appointments a year just to stay alive. What’s the point of living if you’re just going to the doctor every time you blink? I’m just gonna keep using my inhaler and hope for the best. At least I’m breathing.
Palanivelu Sivanathan
Think about it… the lungs… they’re not just organs… they’re the first frontier of the soul’s connection to the cosmos… when we inhale… we don’t just take in oxygen… we take in the breath of the universe… and when we spray chemicals into that sacred passage… we disrupt the natural harmony… the body… it knows… it remembers… the ancient rhythm… and when we silence it with synthetic steroids… we are not healing… we are silencing… and silence… is not peace… it is surrender…
…but also… rinse and spit… always…
Write a comment