


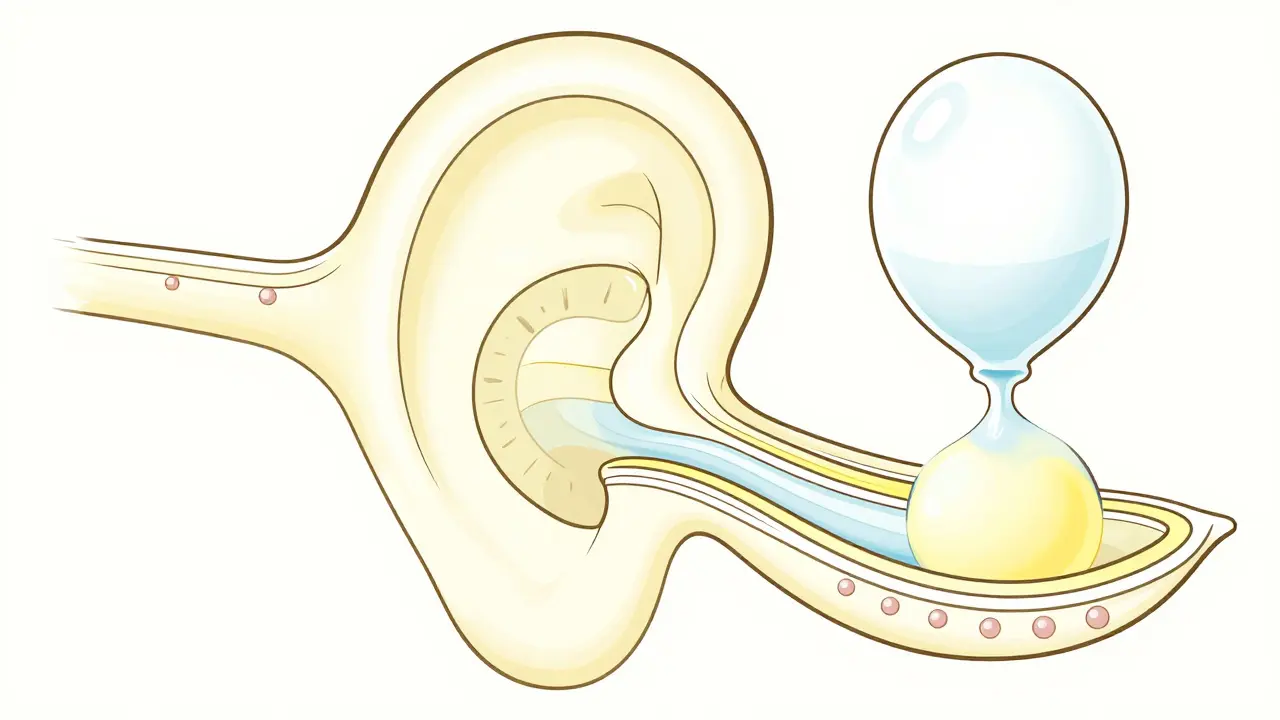
What's Actually Happening Inside Your Ear?
To understand the symptoms, you have to look at the inner ear's plumbing. Your ear uses two distinct fluids to help you balance and hear. First, there is Endolymph is a potassium-rich fluid that fills the membranous labyrinth, including the cochlea and semicircular canals . Then there is perilymph, a sodium-rich fluid that surrounds it. In a healthy ear, these fluids stay balanced. But in Meniere's, you develop Endolymphatic Hydrops is the abnormal accumulation of endolymph fluid that disrupts the ionic balance necessary for hearing and balance . Think of it like a water balloon being overfilled. Eventually, the pressure becomes too much for the delicate membranes to handle. Recent 3D imaging from the Hearing Health Foundation shows that different parts of the ear react differently to this pressure. The saccule is almost always involved (97% of cases), while the utricle is more resilient, only dilating in about 32% of patients. This happens because the membranes in the utricle are naturally thicker, providing more mechanical resistance to the fluid pressure.The Hidden Culprits: Salt, Inflammation, and Genetics
Why does this fluid build up in the first place? There isn't one single answer, but a few key factors play a role. One of the most interesting links is the connection between the inner ear and your kidneys. The structure that produces endolymph, called the stria vascularis, works very similarly to renal tissue. This is exactly why doctors suggest a Meniere's Disease diet low in sodium-usually between 1,500 and 2,000 mg per day-to help reduce fluid production. However, it's not all about salt. New research published in Frontiers in Immunology (2025) suggests that immune dysregulation is a major driver. People with MD show significantly higher levels of inflammatory markers like TNF-α and IL-6. These chemicals break down the blood-labyrinth barrier, allowing T-cells to enter and cause chronic inflammation. This inflammation can lead to fibrotic remodeling, where healthy tissue is replaced by scar tissue, making the fluid drainage system even less efficient.| Contributing Factor | Estimated Prevalence | Primary Mechanism |
|---|---|---|
| Poor Fluid Drainage | 40% | Narrowed endolymphatic ducts |
| Autoimmune Disorders | 25% | T-cell infiltration and inflammation |
| Genetic Predisposition | 20% | SLC26A4 gene mutations (ion channel issues) |
| Viral Infections | 15% | Direct damage to the inner ear lining |
Managing the Symptoms: From Diet to Surgery
Dealing with Meniere's is usually a stepping-stone process. You start with the least invasive options and move toward more aggressive treatments if those fail.- Lifestyle and Diuretics: Reducing salt is the first line of defense. When paired with diuretics like hydrochlorothiazide, some patients see a 22-35% reduction in endolymph volume. However, this only works for about 60% of people because everyone's drainage system is different.
- Steroid Injections: If lifestyle changes aren't enough, doctors may use Intratympanic Corticosteroids is steroid medications injected through the eardrum to reduce inflammation and modulate ion channels . These are effective for about 68-75% of patients in controlling acute vertigo.
- Chemical Ablation: For severe, refractory cases, gentamicin may be injected into the ear. This effectively "turns off" the balance center of that ear. While it controls vertigo in up to 92% of cases, there is a real risk (12-18%) of losing more hearing in that ear.
- Surgical Options: Endolymphatic sac decompression is a surgery designed to relieve pressure. It's decent for stopping vertigo (60-70% success), but it rarely helps recover lost hearing.
The Long-Term Outlook and "Burn Out"
One of the most confusing parts of this disease is that the vertigo attacks can actually stop over time. This isn't always a sign of recovery. In about 38% of patients who have had the disease for over a decade, the inner ear becomes completely filled with fluid. At this point, the pressure stabilizes, and the acute spinning stops, but the damage is done. This state often leads to permanent chronic unsteadiness and severe hearing loss. In fact, 72% of long-term patients experience a loss of more than 50dB in the affected ear. Because of this, early intervention is critical. Using 3D volumetrics to detect hydrops before symptoms even start can help patients begin treatment sooner, potentially saving their hearing.Creating a Comprehensive Management Plan
If you're struggling with these symptoms, a single-pill approach rarely works. The Mayo Clinic found that integrated protocols-combining sodium restriction, diuretics, and immunomodulation-achieve a 78% success rate in symptom control, compared to just 52% for those using only one method. It's also helpful to know that you might have "Vestibular Meniere's." This is a version of the disorder where you get the vertigo but no hearing loss. It accounts for about 18% of cases and often responds better to specific vestibular rehabilitation therapies rather than heavy-duty fluid management.Can I completely cure Meniere's Disease?
Currently, there is no permanent cure that reverses all damage. However, it is highly manageable. Most patients can control their vertigo episodes through a combination of low-sodium diets, diuretics, and medications. The goal is to maintain fluid homeostasis and prevent the permanent loss of hair cells in the cochlea.
Why does a low-salt diet help with ear fluid?
The tissue that produces endolymph in your ear functions similarly to your kidneys. High sodium intake causes the body to retain water, which increases the volume of endolymph. By limiting salt to 1,500-2,000 mg per day, you reduce the osmotic pressure, which can lower fluid production by as much as 37% in some patients.
Is the ringing in my ears (tinnitus) permanent?
Tinnitus in Meniere's is often fluctuating in the early stages, meaning it comes and goes with the fluid pressure. However, as the disease progresses and leads to permanent hair cell loss or fibrotic remodeling of the inner ear, the tinnitus may become constant. Early management of hydrops is the best way to prevent this progression.
What is the difference between a diuretic and a steroid injection?
Diuretics are systemic medications that help your body flush out excess fluid to prevent the "balloon" from overfilling. Steroid injections are local treatments delivered directly into the middle ear. They work by reducing inflammation and modulating the channels that control how fluid moves in and out of the endolymphatic sac.
When should I consider surgery for Meniere's?
Surgery, such as endolymphatic sac decompression, is typically reserved for "refractory" cases-meaning you've tried diet, diuretics, and steroids without success. It is most effective for those whose primary struggle is debilitating vertigo rather than hearing loss, as surgical outcomes for hearing improvement are relatively low (25-35%).
Comments
15 Comments
Betty Kawira
Low sodium is a game changer but honestly, the hardest part is eating out since everything is salted to death.
I've found that prepping your own meals is the only real way to keep it under 2k mg. Just a heads up for anyone starting this-don't forget to check the labels on "healthy" frozen meals, they're usually salt bombs!
prince king
Wow, the way the body balances fluid is just poetry in motion! 🌊✨ It's wild how a little bit of salt can throw the whole system off. Sending good vibes to everyone dealing with the spinning! 🌀🙏
Dale Kensok
The reductionist approach to endolymphatic hydrops presented here is quaint, yet it utterly fails to synthesize the ontological instability of the patient experience. One must analyze the stria vascularis not merely as a renal analog, but as a failure of homeostatic equilibrium within a precarious biological framework. The sheer lack of nuance regarding the epigenetic triggers is frankly embarrassing for anyone claiming a scientific vantage point. Most of the laypeople here are simply absorbing surface-level data without comprehending the systemic failure of the ion-channel architecture. It's an exercise in mediocrity.
Sharon Mathew
ARE YOU KIDDING ME?! 😱 Telling people to just "eat less salt" is such a joke when the post literally says 40% of it is just poor drainage! Like, how does a salad fix a narrowed duct?! This is absolutely ridiculous and totally ignores the trauma of a vertigo attack!
Nigel Gosling
Typical modern medical advice-strip away the soul of the suffering and replace it with a table of percentages. We've become so obsessed with the plumbing of the ear that we've forgotten the existential dread of losing one's balance in a chaotic world. It's a moral failing of our time that we treat humans like leaky faucets. Honestly, the sheer audacity of suggesting a pill is a 'stepping stone' is just peak pharmaceutical arrogance. I'm practically exhausted just reading this sterility.
Stephen Johnson
It's a long road to stability, but there's a certain peace in accepting the unpredictability of it all. Just take it one day at a time.
Jonathan Hall
While I generally appreciate the attempt to bring these medical insights to the public, I find the aggressive push toward surgical interventions somewhat premature and potentially dangerous for those who haven't fully exhausted their non-invasive options. It's important to remember that every body reacts differently to these interventions, and what works for one person might be a complete disaster for another, so we really need to be more cautious about how these success rates are framed. Let's try to keep the conversation balanced and not rush into procedures that can't be undone.
Jarrett Jensen
The terminology employed in this summary is regrettably simplistic. One should have noted that the SLC26A4 mutation is not merely a contributing factor but a primary genetic driver in specific cohorts. The lack of a comprehensive citation list makes the validity of the 2025 trial data highly suspect. It is quite tiresome to encounter such an elementary presentation of complex pathology in a forum that pretends to be informative.
Ryan Wilson
Look at this bunch of clowns pretending they understand pathology. The guy talking about 'ontological instability' probably can't even find his own backside with both hands. It's a bunch of salt-water in your head, get over yourselves and just take the damn meds before you fall over and break a hip. Absolute circus.
Steve Grayson
I agree with the points about the integrated protocols. Using multiple methods definitely seems more reliable than just one.
Abhishek Charan
I must disagree vehemently!!! 😡 The statistics provided are simply too optimistic... and the layout is entirely lacking in rigor!!! 🙄 Why is no one mentioning the psychological toll??? 💥
Jenna Riordan
I have a cousin who had the decompression surgery and she said it didn't do anything for her hearing at all but she stopped spinning. Does anyone know if she should try the steroid injections now or is it too late?
Raymond Lipanog
It is perhaps prudent to consider the intersection of these physiological challenges with the mental fortitude required to endure them. By maintaining a disciplined approach to the low-sodium regimen and accepting the limitations of current medicine, one may find a sustainable equilibrium despite the inherent instability of the condition.
Angela Cook
USA has the best specialists for this! If you're not getting the 3D volumetrics mentioned here, you're probably in the wrong country. We lead the way in inner ear research for a reason!
Kevin Taggart
man those steroid injections sound scary... like actually puttin stuff thru the eardrum? 😬 hope it works tho
Write a comment