


When your doctor finds a lump in your neck, it’s natural to worry. But here’s the truth: thyroid ultrasound isn’t just a scan-it’s your first real clue about whether that lump matters. Over 60% of thyroid nodules are found this way, not by feeling your neck, but by using sound waves to see inside. And what it shows can change everything-from avoiding surgery to catching cancer early.
What Thyroid Ultrasound Actually Shows
Thyroid ultrasound doesn’t use radiation. It uses high-frequency sound waves, like sonar for your body. A probe pressed gently against your neck sends out pulses, then listens for echoes. Those echoes build a real-time image of your thyroid gland. It’s quick, painless, and doesn’t need needles or injections.
But it’s not just about spotting a nodule. The real power is in what it reveals about the nodule’s structure. Five key features are checked every time:
- Composition: Is it full of fluid (cystic)? Mostly solid? Or a mix? Solid parts raise red flags.
- Echogenicity: How bright or dark does it look? Markedly hypoechoic (very dark) nodules are more likely to be cancerous.
- Shape: A nodule that’s taller than it is wide is a major warning sign. Normal nodules are wider than tall.
- Margin: Smooth edges? Good. Jagged, unclear, or spreading outside the thyroid? Trouble.
- Punctate echogenic foci: Tiny white dots inside the nodule. These are microcalcifications-and they’re one of the strongest predictors of cancer.
These aren’t guesses. They’re based on decades of data from hundreds of thousands of biopsies. Each feature gets scored. Add them up, and you get a risk category.
The TI-RADS System: Your Risk Score
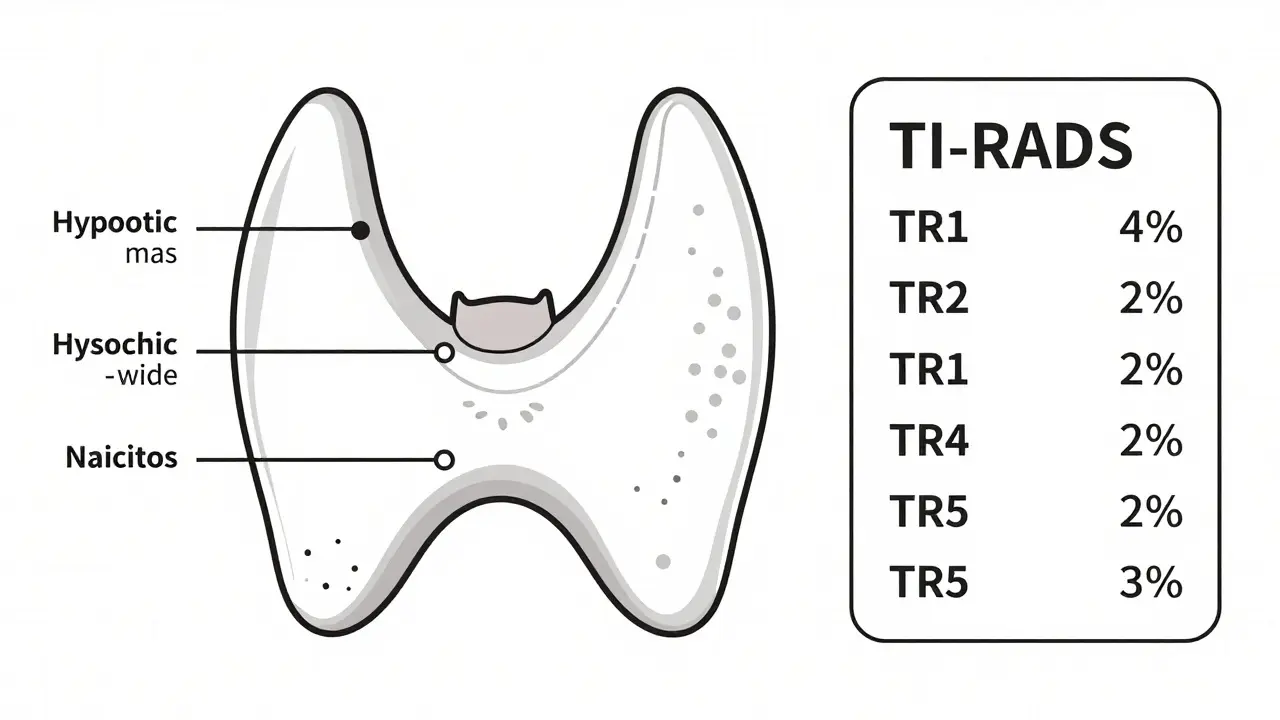
In 2017, the American College of Radiology created TI-RADS-Thyroid Imaging Reporting and Data System. It turned vague descriptions into clear numbers. Here’s how it breaks down:
| TI-RADS Level | Points | Malignancy Risk |
|---|---|---|
| TR1 | 0 | 0.3% |
| TR2 | 2 | 1.5% |
| TR3 | 3 | 4.8% |
| TR4 | 4-6 | 9.1% |
| TR5 | 7+ | 35% |
TR1 and TR2? Almost always harmless. You might never see it again. TR3? Still low risk-monitoring is usually enough. But TR4 and TR5? That’s where biopsy becomes necessary. A nodule scoring TR5 has a 1 in 3 chance of being cancer. That’s not a guess. That’s data.
And size isn’t everything. A 1.5 cm nodule with microcalcifications and irregular borders (TR5) is far more concerning than a 3 cm solid nodule with smooth edges (TR2). Ultrasound tells you why.
Why Ultrasound Beats Other Scans
You might think a CT or MRI gives more detail. But for thyroid nodules, they don’t. CT scans pick up about 30% of nodules. MRI? Only 25%. Ultrasound finds 68%. Why? Because it’s tuned for shallow structures. It sees the fine details other scans miss.
Nuclear scans (like radioactive iodine tests) can tell you if a nodule is "hot" (overactive) or "cold" (underactive). Hot nodules almost never turn cancerous. Cold ones? About 15% risk. But here’s the catch: nuclear scans don’t show shape, margins, or calcifications. They can’t tell you if a nodule is dangerous-they just tell you it’s not functioning normally. And they expose you to radiation.
Ultrasound? No radiation. Real-time. And it guides the biopsy. When a doctor uses ultrasound to steer the needle into a nodule, the chance of getting a useless sample drops from 25% to under 5%. That’s huge. A bad biopsy means a repeat. A repeat means more stress, more cost, more delay.
What Happens After the Scan?
Not every nodule needs a biopsy. Guidelines are clear:
- Under 5 mm: No follow-up needed, even if it looks suspicious. These almost never become dangerous.
- 1 cm or larger + suspicious features (TR4/TR5): Biopsy recommended.
- TR3 nodule (4.8% risk) over 2.5 cm: Biopsy advised. Studies show thyroid cancers under this size rarely spread or cause harm.
Even if a biopsy comes back "indeterminate"-meaning it’s unclear if it’s cancer-ultrasound still rules. You don’t stop watching. You come back every 6 to 12 months. Growth? That’s your signal. No growth? You’re likely fine.
And here’s something surprising: for tiny papillary thyroid cancers (under 1 cm), many doctors now choose active surveillance over surgery. Why? Because 99% of patients live 10 years or more without treatment. Surgery carries risks-nerve damage, lifelong hormone pills. Sometimes, watching is safer.
The New Frontier: AI and Deep Learning
Ultrasound isn’t static. In 2023, a study in Nature Scientific Reports showed a new AI model that analyzed nodule shape, texture, and blood flow. It reached 94.2% accuracy in spotting cancer. Traditional methods? 87.6%. That 6.6% jump isn’t just a number-it means fewer false alarms and fewer missed cancers.
These tools aren’t replacing radiologists. They’re helping them. By highlighting the subtle patterns humans might miss-like a slight asymmetry in blood flow or a barely visible microcalcification-they reduce human error. One study found that when AI was used, inter-observer disagreement dropped from 30% to under 15%.
By 2025, we’ll likely see TI-RADS updated to include AI-assisted scoring. Imagine a system that doesn’t just show you the nodule, but says: "Based on 500,000 similar cases, this has a 12% risk. Here’s why." That’s the future-and it’s already here in top hospitals.
What Goes Wrong? Common Mistakes
Ultrasound is powerful-but only if done right. Here’s where things go off track:
- Missing lymph nodes: About 35% of community scans skip checking the neck for swollen lymph nodes. That’s a blind spot. Cancer spreads there first.
- Using the wrong probe: A probe under 10 MHz can’t show fine details. You need a high-frequency linear probe.
- Not measuring properly: Nodules must be measured in three directions. One measurement isn’t enough to track growth.
- Operator inexperience: It takes 200-300 scans to become consistent. If your scan was done by someone new, ask if they’re certified.
Accredited centers follow strict rules: images saved in two planes, full thyroid and lymph node views, documented measurements. If your clinic doesn’t mention these, it’s worth asking.
What’s Next?
Thyroid cancer rates have tripled since the 1970s. But most of that increase? It’s from finding tiny cancers that would’ve gone unnoticed. Ultrasound didn’t cause the rise-it just made us see it.
The real goal now isn’t to find every single nodule. It’s to find the dangerous ones. And that’s exactly what modern ultrasound, guided by TI-RADS and backed by AI, is doing.
It’s not perfect. Biopsies still happen. Some cancers slip through. But for the vast majority, this scan gives clarity. Not fear. Not guesswork. Just facts.
Can a thyroid ultrasound diagnose cancer?
No. Ultrasound shows features that suggest cancer risk, but it can’t confirm cancer. Only a biopsy can do that. Ultrasound tells you whether a biopsy is needed, and where to aim the needle.
Are all thyroid nodules dangerous?
No. Over 90% of thyroid nodules are benign. Most people have them and never know. The goal isn’t to remove every nodule-it’s to find the small percentage that could become harmful.
How often should I get a follow-up ultrasound?
It depends on the risk level. TR1 and TR2 nodules rarely need follow-up. TR3 nodules under 2.5 cm are usually checked in 1-2 years. TR4/TR5 nodules or those growing over time need more frequent scans-every 6-12 months-or biopsy.
Is thyroid ultrasound safe during pregnancy?
Yes. Ultrasound uses sound waves, not radiation. It’s completely safe during pregnancy and is often used to evaluate thyroid changes that occur in pregnancy.
Can I skip the ultrasound if my thyroid blood tests are normal?
Yes-if you have no symptoms or physical findings. But if a nodule is felt or seen on another scan, ultrasound is still needed. Blood tests show function, not structure. You can have normal thyroid levels and still have a cancerous nodule.
Do I need a referral for a thyroid ultrasound?
In most healthcare systems, yes. It’s typically ordered by an endocrinologist, primary care doctor, or surgeon after a physical exam or abnormal blood test. Some private clinics allow self-referral, but insurance usually requires a referral.